Dermatology
Medicine of the skin, hair, nails, and mucous membranes — spanning medical, surgical, and aesthetic care.
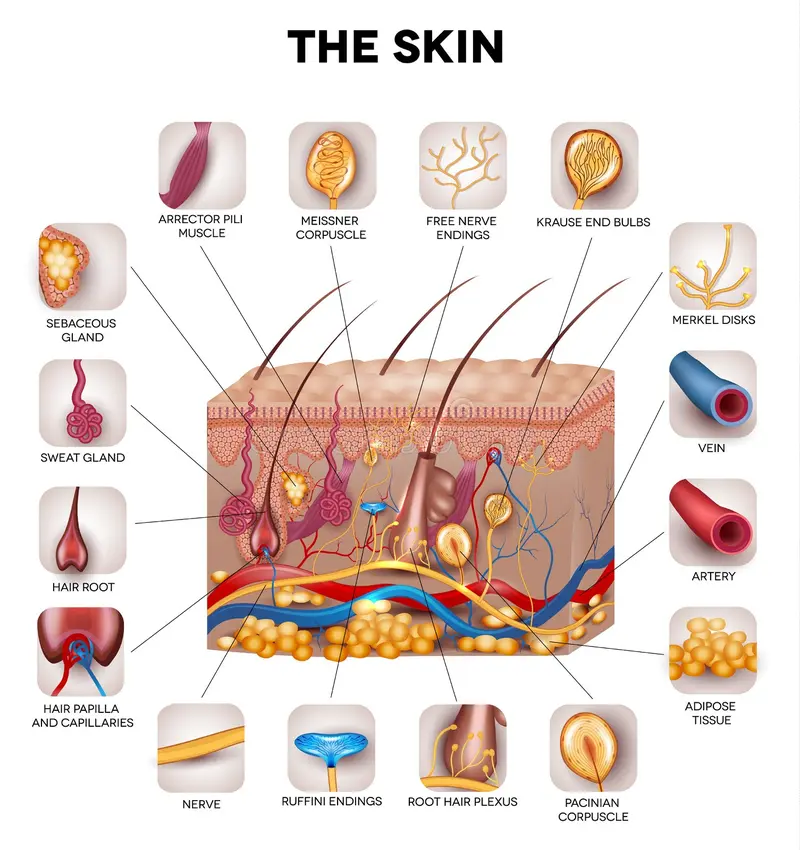
Skin Anatomy
The skin is a layered organ built for barrier defense, sensation, thermoregulation, and immune surveillance.
1) Epidermis
- Outermost layer; barrier function & melanin production
- Cells: keratinocytes, melanocytes, Langerhans cells
2) Dermis
- Collagen, elastin, vessels, nerves, sweat & sebaceous glands
- Provides elasticity, sensation, and thermoregulation
3) Hypodermis (Subcutis)
- Adipose layer for insulation and shock absorption
What Dermatology Covers
Dermatology is the branch of medicine dealing with the skin, hair, nails, and mucous membranes, encompassing both medical and surgical aspects. From the Greek derma (skin) + logia (study), the field addresses >3,000 conditions ranging from cosmetic concerns to life-threatening disease. Given the visibility of skin pathology, dermatology bridges patient-facing clinical care and investigative research.
Dermatologist Training Pathway
| Stage | Typical Duration | Notes |
|---|---|---|
| Medical School | 4 years | MD or DO |
| Internship | 1 year | Usually Internal Medicine or General Surgery |
| Residency | 3+ years | Medical, surgical & cosmetic dermatology |
| Fellowship (optional) | 1–2 years | Peds Derm, Dermatopathology, Mohs, Cosmetics |
Subspecialties: Pediatric • Dermatopathology • Mohs Surgery • Cosmetic
Public Health & Prevention
- Skin cancer screening and early detection programs
- Education on sun protection and self-examinations
- Closing gaps in access and outcomes across skin tones & communities
Common Dermatologic Conditions
Inflammatory
- Eczema (Atopic Dermatitis): Chronic pruritus; atopy association
- Psoriasis: Immune-mediated; erythematous plaques with silvery scale
- Acne Vulgaris: Pilosebaceous disorder; often hormone-modulated
Infectious
- Bacterial: Impetigo, cellulitis
- Fungal: Tinea corporis, candidiasis
- Viral: Herpes simplex, VZV, molluscum
Neoplastic & Pigmentary
- Benign: Seborrheic keratoses, nevi
- Malignant: BCC, SCC, melanoma
- Vitiligo: Autoimmune melanocyte loss
- Melasma: UV & hormone-related hyperpigmentation
Dermatology & Systemic Disease
- Lupus erythematosus: Malar “butterfly” rash may precede systemic involvement
- Diabetes mellitus: Acanthosis nigricans, necrobiosis lipoidica
- Paraneoplastic syndromes: Cutaneous clues to occult malignancy
Diagnostic Techniques
Bedside & Imaging
- Clinical exam & pattern recognition
- Dermoscopy
- Wood’s lamp for pigment & some fungal disorders
Laboratory & Procedures
- Skin biopsy: punch, shave, excisional
- Patch testing for contact dermatitis
- Targeted blood tests: ANA, IgE, autoantibodies
Pattern + Proof
- History + distribution matter as much as morphology
- When in doubt: biopsy early (especially for “weird” rashes)
Treatment Modalities
Topical
- Corticosteroids • Retinoids • Antibiotics/Antifungals
- Calcineurin inhibitors
Systemic
- Immunosuppressants (e.g., methotrexate, cyclosporine)
- Biologics (e.g., adalimumab, ustekinumab)
- Oral antibiotics & antifungals
Procedural & Light
- Cryotherapy • Electrosurgery • Laser therapy
- Excisional surgery • Mohs micrographic surgery
- Narrowband UVB • PUVA (psoralen + UVA)
Skin Types & Sun Safety
Fitzpatrick Skin Phototypes (I–VI)
- I–II: Burns easily, minimal tan → higher UV sensitivity
- III–IV: Sometimes burns, tans uniformly
- V–VI: Rarely burns, deeply pigmented → melanoma can be acral/mucosal; look beyond sun-exposed sites
Sun Protection
- Broad-spectrum SPF 30+ daily; SPF 50+ for prolonged outdoor exposure
- Reapply every 2 hours; UPF clothing; shade 10am–4pm
- Vitamin D: consider dietary/supplement sources as needed
Reality Check
- “Cloudy” doesn’t mean “no UV”
- Neck, ears, hands: the usual SPF graveyard
Skin of Color Considerations
- Inflammation may present with purple/gray/ash tones rather than bright erythema
- Post-inflammatory hyper/hypopigmentation is common; treat inflammation gently to minimize dyspigmentation
- Acral lentiginous melanoma: carefully examine palms/soles/nail beds
- Keloid risk higher — favor silicone gel/sheets & pressure therapy in scar care
Melanoma Recognition
ABCDE
- Asymmetry
- Border irregular
- Color variegation
- Diameter > 6 mm (or evolving smaller)
- Evolving size/shape/color/symptoms
Ugly Duckling & Red Flags
- Lesion unlike the patient’s other moles
- New spot in adulthood; bleeding, non-healing, rapid change
High-Risk Areas
- Palms/soles
- Under nails
- Mucosal sites
Acne Treatment Ladder (Simplified)
- Mild: topical benzoyl peroxide ± retinoid
- Moderate: add topical antibiotic (clindamycin) or oral doxycycline
- Female patients: consider combined OCP or spironolactone for hormonal pattern
- Severe/nodulocystic or scarring: oral isotretinoin with monitoring
Always use non-comedogenic skincare; emphasize adherence and sun safety with retinoids.
Atopic Dermatitis – Step-Up Care
- Baseline: emollients, trigger avoidance, short lukewarm baths, gentle cleansers
- Flares: topical steroids by potency/area; calcineurin inhibitors for sensitive sites
- Refractory/moderate-severe: phototherapy or systemic/biologic therapy per guidelines
- Antihistamines for itch-related sleep issues (symptomatic); treat superinfection promptly
Psoriasis – Assess & Treat
- Severity metrics: BSA, PASI, DLQI for impact
- Comorbidities: arthritis, metabolic syndrome, depression, cardiovascular risk
- Mild: topicals (steroids, vitamin D analogs)
- Moderate–Severe: phototherapy, systemics, or biologics (TNF-α, IL-17/23)
Drug Eruptions & Emergencies
Common Eruptions
- Morbilliform exanthem (often antibiotics)
- Urticaria/angioedema
- Fixed drug eruption (recurrent same site)
SJS/TEN Red Flags
- Facial edema, mucosal erosions (ocular/oral/genital)
- Targetoid lesions, skin pain, rapid progression
- Systemic symptoms (fever, malaise); urgent referral/hospitalization
Do Not “Wait and See”
- Skin pain + mucosa = move fast
- Rapid spread = ER-level urgency
Skin Microbiome & Barrier
- Barrier repair (ceramides, occlusives) reduces TEWL and flares
- Over-sanitization can disrupt commensals; balance cleansing with barrier support
- Diet, stress, and sleep influence inflammation and skin health
Wound & Scar Care Basics
- Clean, moist wound environment promotes re-epithelialization
- Petrolatum for simple wounds; avoid peroxide/iodine on fresh tissue
- Scar modulation: silicone gel/sheets, massage, sun protection; consider laser or injections for hypertrophic/keloid
Teledermatology – Photo Tips
- Good indirect daylight; neutral background; no flash glare
- Include a ruler/coin for scale; take overview + close-ups
- Capture color faithfully; avoid heavy filters/makeup on the area
Recent Advances
- Biologics: Transformative outcomes in psoriasis & hidradenitis suppurativa
- Teledermatology: Access expansion for rural/underserved populations
- AI in Dermatology: Decision support & melanoma screening assistance
- Gene & Stem-cell Therapies: Emerging options for rare genetic skin disease