All the Different Arrhythmias: The Heart’s Many Offbeat Grooves
Your heart’s electrical system is usually smooth and rhythmic—until it isn’t. Below, each arrhythmia gets its own quick-read section with what it is, how it looks on EKG, and why it matters.
SinusAtrialJunctionalAV BlockVentricularChannelopathies
1) Sinus Arrhythmia Usually benign
| What it is | Respiratory-linked rate variation—speeds with inspiration, slows with expiration. |
|---|---|
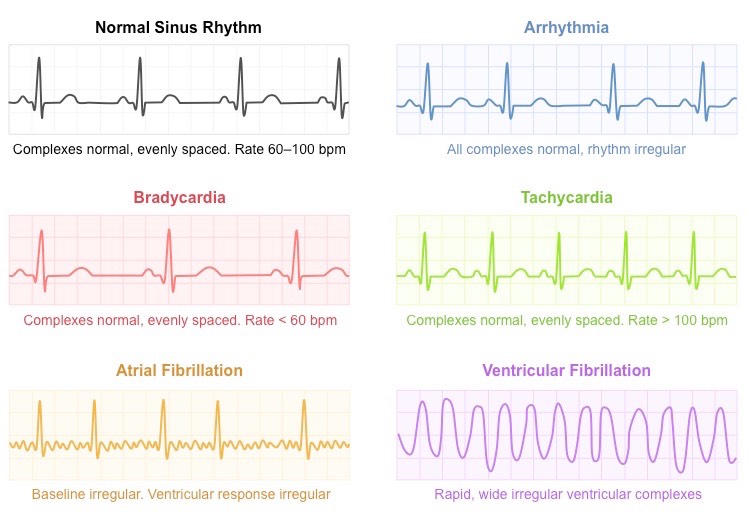
| EKG | Normal P and QRS; slight beat-to-beat RR variability. |
| Clinical | Common in healthy young people; no treatment needed. |
2) Sinus Bradycardia
| What it is | Sinus rate <60 bpm. |
|---|---|
| EKG | P before each QRS; normal conduction but slow. |
| Clinical | Normal in athletes/sleep; symptomatic cases (fatigue, syncope) prompt evaluation of drugs, hypothyroidism, or sinus node disease. |
3) Sinus Tachycardia
| What it is | Sinus rate >100 bpm due to exercise, fever, anemia, sepsis, pain, hyperthyroidism, etc. |
|---|---|
| EKG | Normal P/QRS at a faster rate. |
| Clinical | Treat the cause; inappropriate sinus tachycardia is a diagnosis of exclusion. |
4) Premature Atrial Contractions (PACs) Usually benign
| What it is | Early atrial beats outside the sinus node. |
|---|---|
| EKG | Early, differently shaped P wave ± non-compensatory pause; normal QRS. |
| Clinical | Often incidental; may herald atrial tachyarrhythmias in some patients. |
5) Premature Ventricular Contractions (PVCs)
| What it is | Early ventricular beats. |
|---|---|
| EKG | Wide, bizarre QRS not preceded by P; typically a compensatory pause. |
| Clinical | Common; frequent or symptomatic PVCs warrant assessment for structural disease; consider burden-related cardiomyopathy if very frequent. |
6) Atrial Fibrillation (AFib)
| What it is | Chaotic atrial activity with loss of organized contraction. |
|---|---|
| EKG | No distinct P waves; irregularly irregular RR intervals. |
| Clinical | ↑ Stroke risk → assess CHA2DS2-VASc for anticoagulation; rate vs rhythm control; risk-factor management (sleep apnea, alcohol). |
7) Atrial Flutter
| What it is | Rapid macro-reentry in atria (often ~300 bpm). |
|---|---|
| EKG | “Sawtooth” flutter waves; often 2:1 AV conduction (~150 bpm). |
| Clinical | Ablation is frequently curative; stroke prevention parallels AFib strategy. |
8) Supraventricular Tachycardia (SVT)
| What it is | Paroxysmal narrow-complex tachycardia, often AVNRT/AVRT. |
|---|---|
| EKG | Regular, narrow QRS >150 bpm; P waves hidden/retrograde. |
| Clinical | Vagal maneuvers, adenosine for diagnosis/termination; ablation for recurrent episodes. |
9) Ventricular Tachycardia (VT)
| What it is | Fast ventricular rhythm (monomorphic or polymorphic). |
|---|---|
| EKG | Wide QRS tachycardia; AV dissociation/capture or fusion beats support VT over SVT with aberrancy. |
| Clinical | Potentially life-threatening; evaluate for ischemia/structural disease; ACLS protocols; ICD consideration if sustained or high risk. |
10) Ventricular Fibrillation (VF)
| What it is | Chaotic ventricular activation without output. |
|---|---|
| EKG | Irregular, erratic waveform with no identifiable QRS. |
| Clinical | Cardiac arrest—immediate defibrillation and ACLS. |
11) First-Degree AV Block Usually benign
| What it is | Delayed AV node conduction. |
|---|---|
| EKG | PR > 200 ms; all P conducted. |
| Clinical | Often incidental; monitor for symptoms or progression. |
12) Second-Degree AV Block (Type I, Wenckebach)
| What it is | Progressive PR prolongation until a beat drops. |
|---|---|
| EKG | Longer-longer-drop pattern. |
| Clinical | Often AV nodal and benign; observe unless symptomatic. |
13) Second-Degree AV Block (Type II)
| What it is | Intermittent non-conducted P waves with constant PR in conducted beats. |
|---|---|
| EKG | Dropped QRS without preceding PR lengthening. |
| Clinical | Infranodal—higher risk of complete block; pacemaker usually indicated. |
14) Third-Degree (Complete) Heart Block
| What it is | No atrioventricular conduction. |
|---|---|
| EKG | P–QRS dissociation; escape rhythm maintains rate. |
| Clinical | Severe bradycardia/syncope; pacemaker required. |
15) Bundle Branch Blocks (RBBB/LBBB)
| What it is | Delay/block in right or left bundle. |
|---|---|
| EKG | Wide QRS; RBBB rsR′ in V1; LBBB broad/notched R in I, aVL, V5–V6. |
| Clinical | May indicate structural heart disease (esp. LBBB) and alters ischemia interpretation. |
16) Torsades de Pointes
| What it is | Polymorphic VT with “twisting” QRS around the baseline; associated with prolonged QT. |
|---|---|
| EKG | Irregular, varying-amplitude wide complexes. |
| Clinical | Emergency: IV magnesium, correct electrolytes; stop QT-prolonging drugs; overdrive pacing if unstable. |
17) Junctional Rhythm
| What it is | AV junction takes over pacemaking when sinus fails or conduction impaired. |
|---|---|
| EKG | Absent or inverted P, narrow QRS, regular rhythm. |
| Clinical | May be benign or reflect sinus node disease/drug effect. |
Brugada Syndrome SCD risk
| What it is | Inherited sodium-channelopathy (often SCN5A) predisposing to malignant ventricular arrhythmias, often in structurally normal hearts. |
|---|---|
| EKG | Type 1 coved ST-segment elevation >2 mm in V1–V2 with negative T wave; pattern may be unmasked by fever or sodium-channel blockers. |
| Clinical | Syncope or nocturnal agonal respirations; manage fevers aggressively; avoid offending drugs; ICD for secondary prevention or high-risk profiles. |
Long QT Syndrome (LQTS) Torsades risk
| What it is | Congenital or acquired repolarization disorder prolonging QTc. |
|---|---|
| EKG | QTc prolonged for age/sex; T-wave morphology varies by genotype. |
| Clinical | Syncope with exertion/emotion/rest depending on genotype; avoid QT-prolonging drugs, correct electrolytes; beta-blockers first-line; ICD in high-risk. |
Catecholaminergic Polymorphic VT (CPVT) Exertional syncope
| What it is | Inherited calcium-handling disorder (e.g., RYR2) with adrenergically triggered bidirectional/polymorphic VT. |
|---|---|
| EKG | Normal resting ECG; exercise or stress induces ventricular ectopy → bidirectional/polymorphic VT. |
| Clinical | Beta-blockers (non-selective), flecainide; ICD for survivors; strict trigger avoidance. |
Hypertrophic Cardiomyopathy (HCM) SCD in youth
| What it is | Genetic myocardial disease with LV hypertrophy and myofiber disarray. |
|---|---|
| EKG | LVH patterns, deep narrow Q waves in inferolateral leads, repolarization changes. |
| Clinical | Exertional syncope, dyspnea; risk-stratify for ICD; avoid dehydration and extreme exertion without evaluation. |
Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC)
| What it is | Desmosomal gene variants with fibrofatty RV replacement → VT/VF. |
|---|---|
| EKG | T-wave inversions V1–V3; epsilon waves in some; ventricular arrhythmias of RV origin. |
| Clinical | Exercise restriction; ICD for high risk; family screening. |
Wolff–Parkinson–White (WPW) / Pre-excitation
| What it is | Accessory pathway enabling AV re-entry tachycardias; risk of AF with rapid conduction. |
|---|---|
| EKG | Short PR, delta wave, wide QRS in sinus rhythm. |
| Clinical | Consider ablation; avoid AV-nodal blockers in AF with WPW; use pathway-blocking strategies. |
How This Helps You
Recognizing rhythm patterns + symptoms guides urgency and next steps—when to seek emergency care (e.g., syncope with exertion, chest pain, severe palpitations), what tests your clinician might order (ECG, Holter/patch monitor, echo, stress test, electrolytes, thyroid labs), and how treatment choices are made (medications, ablation, devices, risk-factor control).
Educational only and not a substitute for clinical care. If you have concerning symptoms, seek medical evaluation.
Selected References
- 2023–2024 AHA/ACC/HRS guidance on atrial fibrillation, ventricular arrhythmias, and sudden cardiac death.
- NIH/NCBI Bookshelf & StatPearls chapters on ECG interpretation and arrhythmias.
- UpToDate topic reviews for Brugada syndrome, LQTS, CPVT, HCM, and ARVC.